The term ‘sulfur allergy’ is misleading. It can lead to patients believing that they are allergic to all sulfur-containing medications or preservatives, and even to sulfur, an important building block of life. It can also cause potentially useful medicines to be unnecessarily avoided. The term can be divided into the following 3 groups:
Antibiotic sulfonamides
Non-antibiotic sulfonamides
Sulfur, sulfites & sulfates
Most commonly implicated group associated with allergy.
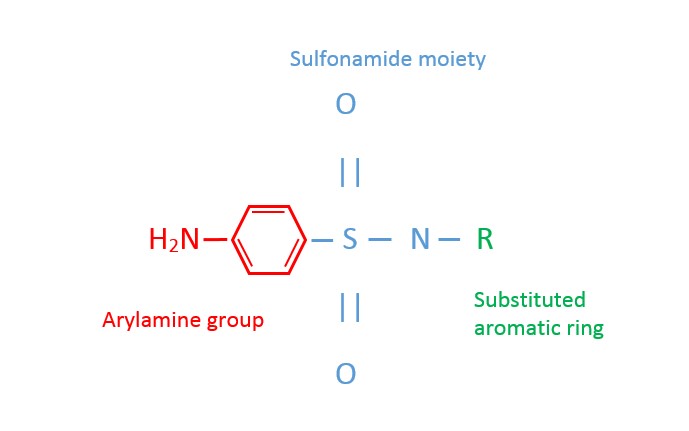
Antibiotic sulfonamides contain an arylamine group (see structure below) that undergoes metabolic changes implicated in the development of hypersensitivity reactions.
The incidence of antibiotic sulfonamide allergy is 1.5-3% of the general population, but can be very high in patients with HIV (up to 60%).
Hypersensitivity reactions most commonly present as fever and morbilliform rash, sometimes with organ involvement, beginning 1-2 weeks after starting therapy.
Cross-reactivity within this group may occur.
see table below (not exhaustive).
Non-antibiotic sulfonamides do not contain an arylamine group and are associated only rarely with hypersensitivity reactions.
Available evidence does not support the existence of cross-reactivity between antibiotic and non-antibiotic sulfonamides.
It is reasonable to use non-antibiotic sulfonamides (e.g. loop diuretics, thiazides, sulfonylureas or triptans) in most patients who are allergic to antibiotic sulfonamides. However, patients allergic to one drug are more likely to be allergic to another, regardless of chemical structure.
see table below (not exhaustive).
Sulfur, sulfites and sulfates do not need to be avoided in patients who have had allergic reactions to sulfonamides (antibiotic or non-antibiotic).
Sulfur is a natural element, to which allergy does not occur.
Sulfite allergy occurs in its own right. Sulfites can induce anaphylaxis, rash, asthma, seizures and death in sensitive patients. Approximately 10% of asthmatics are sulfite sensitive. Sulfites are used to preserve food, beverages and pharmaceuticals.
Sulfate allergy is extremely rare. Sulfates can be mildly irritant and are found in a variety of pharmaceuticals and commonly used substances such as soaps, detergents and cosmetics.
To prevent confusion, the general term ‘sulfur allergy’ should not be used. Please record the name of the drug and nature of the reaction. Adverse drug reactions (ADRs) should not be attributed to classes or groups of drugs (electronic ADR systems, such as MedChart, will alert for “related” drugs). If the drug causing the ‘sulfur allergy’ cannot be identified, it is possible the allergy was to an antibiotic sulfonamide as these are most commonly implicated. Remember, patients allergic to one drug are more likely to be allergic to another, regardless of chemical structure.

 Download PDF
Download PDF